

Monday, 24 November 2014
Friday, 21 November 2014
Cases of Ebola Diagnosed in the United States
- October 23, 2014 - The New York City Department of Health and Mental Hygiene reported a case of Ebola in a medical aid worker who had returned to New York City from Guinea, where the medical aid worker had served with Doctors Without Borders.
- The diagnosis was confirmed by CDC on October 24.
- The patient has recovered and was discharged from Bellevue Hospital Center on November 11.
- October 15, 2014 – A second healthcare worker who provided care for the index patient at Texas Presbyterian Hospital tested positive for Ebola.
- This second healthcare worker was transferred to Emory Hospital in Atlanta, Georgia.
- The healthcare worker had traveled by air from Dallas to Cleveland on October 10 and from Cleveland to Dallas on October 13. CDC worked to ensure that all passengers and crew on the two flights were contacted by public health professionals to answer their questions and arrange follow up as necessary.
- The patient has since recovered and was discharged on October 28.
- By November 3, all passengers on both flights completed the 21-day monitoring period.
- October 10, 2014 – A healthcare worker at Texas Presbyterian Hospital who provided care for the index patient tested positive for Ebola.
- The healthcare worker was isolated after the initial report of a fever and subsequently moved to the National Institutes for Health (NIH) Clinical Center.
- The patient has since recovered and was discharged on October 24.
- September 30, 2014 – CDC confirmed the first laboratory-confirmed case of Ebola to be diagnosed in the United States in a man who had traveled to Dallas, Texas from Liberia.
- The man did not have symptoms when leaving Liberia, but developed symptoms approximately four days after arriving in the United States.
- The man sought medical care at Texas Presbyterian Hospital of Dallas after developing symptoms consistent with Ebola. Based on his travel history and symptoms, CDC recommended testing for Ebola. The medical facility isolated the patient (i.e., index patient) and sent specimens for testing at CDC and at a Texas laboratory.
- Local public health officials identified all close contacts of the index patient for daily monitoring for 21 days after exposure.
- The patient passed away on October 8.
- By November 7, all contacts of the patient completed the 21-day monitoring period.
CDC recognizes that any case of Ebola diagnosed in the United States raises concerns, and any death is too many. Medical and public health professionals across the country have been preparing to respond to the possibility of additional cases. CDC and public health officials in Texas, Ohio, and New York are taking precautions to identify people who had close personal contact with the patients, and healthcare professionals have been reminded to use meticulous infection control at all times.
2014 Ebola Outbreak in West Africa - Outbreak Distribution Map
Countries with Cases of Ebola
| Countries with widespread transmission1 | Affected areas |
|---|---|
| Guinea | Entire country |
| Liberia | Entire country |
| Sierra Leone | Entire country |
| Countries with an initial case or cases and/or localized transmission | Affected areas |
|---|---|
| Mali2 | Kayes, Kourémalé, and Bamako |
| United States3 | Dallas, TX, New York City |
| Previously affected countries4 | Affected areas |
|---|---|
| Nigeria | Lagos, Port Harcourt |
| Senegal | Dakar |
| Spain | Madrid |
Travelers arriving from all areas of Guinea, Liberia, and Sierra Leone are at risk for exposure to Ebola virus.
A single Ebola case was imported from Guinea and was diagnosed in Kayes, Mali on October 23, 2014; no further transmission was associated with this case. Investigation of localized Ebola transmission in Kourémalé and Bamako, following a separate importation from Guinea is currently underway.
One travel-associated Ebola case was imported from Liberia to Dallas, and resulted in transmission to two healthcare workers. One travel-associated Ebola case in a healthcare worker was imported to New York City from Sierra Leone, and did not result in further transmission. Travelers to Dallas or New York City are not at risk for exposure to Ebola.
These countries are currently Ebola-free.
One international importation of Ebola to Nigeria from Liberia resulted in localized transmission (20 cases and 8 deaths), which has ceased.
A single Ebola case in Senegal was imported from Guinea, and did not result in further transmission.
A single Ebola case occurred in a Spanish healthcare worker caring for an Ebola patient who had been transported to Spain from Liberia for care, and did not result in further transmission.
Travelers to Nigeria, Senegal, and Spain are not at risk for exposure to Ebola.
One international importation of Ebola to Nigeria from Liberia resulted in localized transmission (20 cases and 8 deaths), which has ceased.
A single Ebola case in Senegal was imported from Guinea, and did not result in further transmission.
A single Ebola case occurred in a Spanish healthcare worker caring for an Ebola patient who had been transported to Spain from Liberia for care, and did not result in further transmission.
Travelers to Nigeria, Senegal, and Spain are not at risk for exposure to Ebola.
Monday, 17 November 2014
Diagnosis
Diagnosing Ebola in a person who has been infected for only a few days is difficult because the early symptoms, such as fever, are nonspecific to Ebola infection and often are seen in patients with more common diseases, such as malaria and typhoid fever.
However, if a person has the early symptoms of Ebola and has had contact with the blood or body fluids of a person sick with Ebola; contact with objects that have been contaminated with the blood or body fluids of a person sick with Ebola; or contact with infected animals, they should be isolated and public health professionals notified. Samples from the patient can then be collected and tested to confirm infection.
Ebola virus is detected in blood only after onset of symptoms, most notably fever, which accompany the rise in circulating virus within the patient's body. It may take up to three days after symptoms start for the virus to reach detectable levels. Laboratory tests used in diagnosis include:
| Timeline of Infection | Diagnostic tests available |
|---|---|
| Within a few days after symptoms begin |
|
| Later in disease course or after recovery |
|
| Retrospectively in deceased patients |
|
Saturday, 15 November 2014
Epidemiologic Risk Factors to Consider when Evaluating a Person for Exposure to Ebola Virus
The following epidemiologic risk factors should be considered when evaluating a person for Ebola virus disease (Ebola), classifying contacts, or considering public health actions such as monitoring and movement restrictions based on exposure.
- High risk includes any of the following:
- Percutaneous (e.g., needle stick) or mucous membrane exposure to blood or body fluids of a person with Ebola while the person was symptomatic
- Exposure to the blood or body fluids (including but not limited to feces, saliva, sweat, urine, vomit, and semen) of a person with Ebola while the person was symptomatic without appropriate personal protective equipment (PPE)
- Processing blood or body fluids of a person with Ebola while the person was symptomatic without appropriate PPE or standard biosafety precautions
- Direct contact with a dead body without appropriate PPE in a country with widespread Ebola virus transmission
- Having lived in the immediate household and provided direct care to a person with Ebola while the person was symptomatic
- Some risk includes any of the following:
- In countries with widespread Ebola virus transmission:
- direct contact while using appropriate PPE with a person with Ebola while the person was symptomatic or with the person's body fluids
- any direct patient care in other healthcare settings
- Close contact in households, healthcare facilities, or community settings with a person with Ebola while the person was symptomatic
- Close contact is defined as being for a prolonged period of time while not wearing appropriate PPE within approximately 3 feet (1 meter) of a person with Ebola while the person was symptomatic
- In countries with widespread Ebola virus transmission:
- Low (but not zero) risk includes any of the following:
- Having been in a country with widespread Ebola virus transmission within the past 21 days and having had no known exposures
- Having brief direct contact (e.g., shaking hands) while not wearing appropriate PPE, with a person with Ebola while the person was in the early stage of disease
- Brief proximity, such as being in the same room for a brief period of time, with a person with Ebola while the person was symptomatic
- In countries without widespread Ebola virus transmission: direct contact while using appropriate PPE with a person with Ebola while the person was symptomatic
- Traveled on an aircraft with a person with Ebola while the person was symptomatic
- No identifiable risk includes:
- Contact with an asymptomatic person who had contact with person with Ebola
- Contact with a person with Ebola before the person developed symptoms
- Having been more than 21 days previously in a country with widespread Ebola virus transmission
- Having been in a country without widespread Ebola virus transmission and not having any other exposures as defined above
- Aircraft or ship crew members who remain on or in the immediate vicinity of the conveyance and have no direct contact with anyone from the community during the entire time that the conveyance is present in a country with widespread Ebola virus transmission
Friday, 14 November 2014
Risk of Exposure
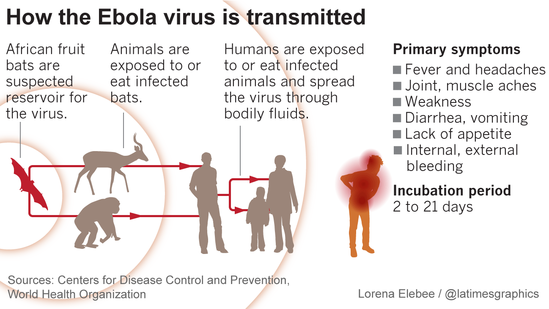
 Ebola viruses are found in several African countries. Ebola was first discovered in 1976 near the Ebola River in what is now the Democratic Republic of the Congo. Since then, outbreaks of Ebola among humans have appeared sporadically in Africa.
Ebola viruses are found in several African countries. Ebola was first discovered in 1976 near the Ebola River in what is now the Democratic Republic of the Congo. Since then, outbreaks of Ebola among humans have appeared sporadically in Africa.Risk
Healthcare providers caring for Ebola patients and family and friends in close contact with Ebola patients are at the highest risk of getting sick because they may come in contact with the blood or body fluids of sick patients. People also can become sick with Ebola after coming in contact with infected wildlife. For example, in Africa, Ebola may spread as a result of handling bushmeat (wild animals hunted for food) and contact with infected bats. The virus also can be spread through contact with objects (like clothes, bedding, needles, syringes/sharps or medical equipment) that have been contaminated with the virus.
Past Ebola Outbreaks
Past Ebola outbreaks have occurred in the following countries:
- Democratic Republic of the Congo (DRC)
- Gabon
- South Sudan
- Ivory Coast
- Uganda
- Republic of the Congo (ROC)
- South Africa (imported)
Subscribe to:
Comments (Atom)